Ricochet is the best place on the internet to discuss the issues of the day, either through commenting on posts or writing your own for our active and dynamic community in a fully moderated environment. In addition, the Ricochet Audio Network offers over 50 original podcasts with new episodes released every day.
 Two Things to Remember About Health Care Policy
Two Things to Remember About Health Care Policy

 When trying to formulate a logical, humane health care system, the key is to start from this fundamental understanding: In our wealthy Western countries, we’re not going to let people die in the streets because they can’t afford readily available health care treatments.
When trying to formulate a logical, humane health care system, the key is to start from this fundamental understanding: In our wealthy Western countries, we’re not going to let people die in the streets because they can’t afford readily available health care treatments.
Since everyone knows we aren’t going to turn people away from emergency rooms, a completely free market won’t work. The free rider problem is insurmountable. People can and will choose not to participate in the market until they become sick, and they will then rely on the good will of society to care for them. So the government will be involved in the health care delivery system in some way. Given the free rider problem, it should do so realistically: It should help people at the bottom while keeping government distortion of the market to a minimum.
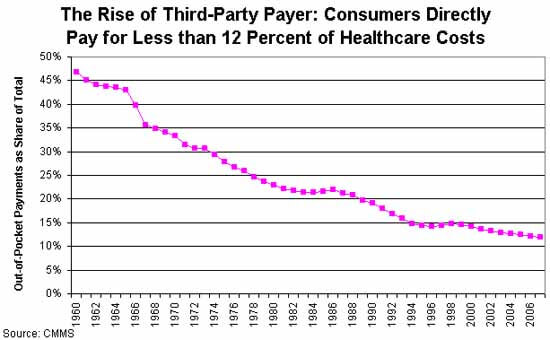 The next thing to consider is the big question: Why is health care so expensive? There’s widespread agreement that third-party payment through insurers is the main problem. There’s no cost control, because neither doctors nor their patients have any incentive to control costs. The only way to gain control over costs is to increase bureaucratic oversight – which adds to the cost.
The next thing to consider is the big question: Why is health care so expensive? There’s widespread agreement that third-party payment through insurers is the main problem. There’s no cost control, because neither doctors nor their patients have any incentive to control costs. The only way to gain control over costs is to increase bureaucratic oversight – which adds to the cost.
Given these two broad parameters, it seems to me that a free-market health care system (or one that’s as free as possible given the first constraint) should begin with universal, single-payer, catastrophic coverage only insurance. That insurance should be very limited in scope to minimize the third-party payer problem.
In a universal catastrophic insurance system, the government would pick up your health care costs, but only if your health care problems reached a threshold such that they were a very significant hardship. This would prevent casual abuse of the system, and it would keep government costs low by eliminating the coverage of routine medical expenses. So: no coverage for routine exams, birth control, small procedures – the things that make up a huge percentage of costs, but should never be paid via an inefficient insurance system. And nothing at all should be covered until you hit your deductible.
To make this palatable to progressives, you can raise the deductible in tandem with income. So a person who makes $20,000 a year might only have to pay for health care until the bills hit $2,000 in a year; a person making $200,000 might be responsible for the first $20,000. Bill Gates might be responsible for the first billion. The numbers and time limits could be negotiated. The important point is that you are responsible for your own health care, but if faced with a health emergency that would bankrupt you, the government will step in. A progressive scheme like this would push more health care into the free market, rather than increasing the scope of government.
Now, would this mean that people would have to pay the deductible out of pocket? Of course not. Employers can offer gap insurance, as can private insurers, on an open market. Gap insurance is much less expensive than full insurance because the insurer’s risk is capped. Pre-existing conditions only cost them up to the cap, so the premium for those would be lower. Because the insurer’s liability is lower for lower-income people (because the cap is lower), insurance would be less expensive for the poor.
People who wish to self-insure could open a HSA and save, say, five times their annual deductible, completely tax-free. This would encourage more people to self-insure to cover the gap, and keep even more of the market out of the third-party payer economy.
This plan would be similar to the health care system in Singapore, a country that spends far less than the US as a proportion of GDP on healthcare, and arguably provides better health care. Singapore also adds a mandatory health savings account, Medisave, to ensure people save enough to pay for the deductible.
Comments?
Published in Domestic Policy, General
It only covers 100% of the catastrophic care plans if the insurance companies can keep the cost of the plan at the cost of the tax credit. That’s a pretty big incentive.
But even if it doesn’t work to control costs — because everyone figures that if costs go up politics will force the tax credit amount up — don’t you have that identical problem with single payer?
I haven’t read the next pages of comments, but unless you factor in all of the additional government regulations that go into medical care–including medical malpractice–you aren’t comparing apples to apples.
I’d say that is true, people don’t save for the unexpected, because they have ‘insurance.’
Dan,
Your Humira example is a good example of why third party payer drives up costs. The only reason why they can charge $3000 /mo for a treatment is that the cost is subsidized by others. If people had to pay for the whole cost the demand would be much less and the price would either go down or the number of units would go way down. In either case the profit of the drug company would be much less.
My own preference is for the government to setup public hospitals. These hospitals would be free to all comers, would give marginal care, and have to strongly ration their patient care. This would give everybody free basic medical care if you really need it. Along side this unleash the private medical market. I would expect this system would quickly drive costs down to be affordable for most people.
This is true in most of the developed world – certainly so in Australia.
They aren’t poorly paid here either.
While ours drives them down. Perhaps worth exploring?
I’ll go further – DocJay should be paid more because he’s worth it.
I think we bill by procedure over here too, so that is not the difference between the systems.
We won’t. For better or worse, that won’t happen.
Dan, I’m (deliberately) not talking about pharmaceuticals, I gave a link which compared the price of surgical procedures.
Example: Angioplasty cost
Australia: $8,911
US: from $16,533 to $61,649; average cost: $28,182
How much of this is due to different pharmaceutical prices?
I know people have dismissed the benefit to consumers of the bargaining power of single payer systems, claiming that private insurance companies can achieve the same or better results.
From the Washington Post, however:
I agree with you that single payer should not be the only game in town – imho single payer covering everything to a basic minimum (paid for by a universal levy, and available to everybody on the basis of need) complemented by private insurance (which gives more choice about timing and physician) combines the best of both worlds.
Would I go to India for my heart bypass surgery if I didn’t have good insurance in the U.S. that will pay for it? Yes, I would, even though the follow-up care would be very difficult. Somehow we have to make this work so that we’re competitive with India.
It doesn’t matter if it’s pharmaceuticals or surgical procedures – the price for something is determined by what the market will bear. And every market is different.
If America has a higher percentage of wealthy people, that could drive up the decision to raise prices. Or perhaps medical regulations and bookkeeping fees are higher. Or doctors have to be paid more to attract them to the local market.
As an example, American software developers make on average something like 30% more than do Canadian software developers – even if they went to the same schools and even if the Canadians perform better. Why? Because that’s the way the market shakes out. Sometimes it’s even hard to pinpoint a reason. Cost of living, access to markets, difficulty of remote management, whatever. The price generally is what it is, and neither the buyer or seller have much control over it. Try to offer less, and you won’t find good employees. Offer more, and you over-pay and your competitors eat your lunch.
That said, it’s always worth looking for systemic factors that can affect price. In the U.S. there so many distortions of the health care marketplace due to government policy that it’s hard to know where to even start.
Or there’s no single payer that can bargain powerfully for all consumers?
No, there isn’t. Because if there is only a single payer, there is no more market.
Sorry, systems like Australia prove you wrong.
Edited to add: single payer is perhaps misleading. There is a universal insurer, which can be augmented if you wish with additional insurance. Seems to work.
If you have a single entity bargaining for a product, it’s not bargaining. There may be some successful aspects to it, but it’s not bargaining in a market sense.
Even when it isn’t all-powerful… I have seen buying collectives for other products, say computer gadgets – that I was urged to use because my organization was part of the collective – but which very seldom steered me to the best price or level of service. They worked well in the eyes of some people, but not for persons like me who had to do the best for his department that he could with the available funds.
There are reasons a purchasing collective does not usually succeed as well as individual consumers do. There is a literature on the history of these in the United States, e.g. in the days of agrarian protest, but this is a field where much historical research remains to be done.
I get that, and I don’t doubt your examples of buying collectives for other products, but when it comes to buying angioplasties this approach really seems to outperform the others for the consumer.
I understand why free market theory tells me it shouldn’t outperform other approaches, but the cost figures indicate that it does.
I’m just not convinced that one should support a less successful approach for ideological reasons.
No, but it might be good if it makes me skeptical enough to want to understand the situation a lot better before agreeing that it’s wonderful enough and sustainable enough to apply to us. I mean, there are people here in the United States who think our Social Security system is great. I’d hope an outsider would want to know just what makes it so great before agreeing.
Well I hope it’s piqued your interest, and yes, your point about surface vs content is taken.
Both sides of this argument are entirely missing the point. Zafar, what you don’t understand is that, despite our protestations to the contrary, US pricing is set almost entirely by a single government payer: Medicare. The problem is not that prices are too high in the US and appropriate in Australia, the problem is that innovation has not functioned to drive prices down in either place because of the interventions of government in the health care marketplace. The differences in prices between Australia and the US don’t have anything to do with the single payer system in Australia, because, systematically, government meddling has had the same general effect in both places.
Sad I missed this conversation yesterday. Dan, nice job in sketching out some of the realistic constraints our society puts on the freedom of the healthcare market, and proposing some realistic ways of coping with those realities.
From reading the comments, it seems there are two huge points that are not visible to most people who do not actually work in the healthcare system:
1) The “dying in the streets” scenario is not about emergency care, but about chronic care and end-of-life treatment for the elderly. Those two categories eat up much, much more of our healthcare spending than someone who goes to the emergency room for antibiotics (or even a car accident) because they have no insurance and can’t afford an office visit. However, the number of patients who fall into this category is small enough that most people usually aren’t even aware they exist.
2) As has been mentioned several times, at its heart America does have a single-payer system: it’s called Medicare. If Medicare were it’s own country, it would be one of the largest single-payer systems in the world. Yet Medicare has many fewer cost-control measures than most deliberate single-payer systems.
If you give me some good words to search for (and I might search for peer-reviewed studies via Jstor as well as the usual google) I might have a little time to study further. I’d like to learn more details of how health care systems work in other countries. One advantage of studying Australia is that I almost know the language.
If there are personal names associated with any initiatives or controversies, that might help me home in on the interesting stuff. Also terms that are used in public controversies and such.
How, pray tell, is charitable giving NOT in keeping with a free market? How is a hospital system marking up costs for those who can pay a full price to account for those who cannot or do not NOT in keeping with a free market? How is pursuing remedy against those who ultimately do not pay NOT in keeping with a free market?
WTH is it today with health care anti-freemarketeers puking logical fallacy all over Ricochet?
WTH is it with people championing the ‘free market’ who don’t seem to understand what it is?
Giving out freebies, and then charging them to someone else under the table and without their agreement is not a ‘free market’ transaction. It’s a market externality and an example of market FAILURE.
You won’t find many people more supportive of a free market than me. But I’m also a pragmatist. Any health care policy proposal that starts with, “Hey, the poor can depend on the kindness of strangers for their health” is a NON-STARTER in today’s world. That’s just a fact. No one will listen to your proposal unless it has some mechanism for providing health care to people who cannot afford it.
Therefore, the challenge is not to come up with a plan for destroying all government influence in health care. The challenge is to find a health care policy that minimizes government influence as much as possible while still being saleable to voters.
It’s easy to say, “Burn it all down! Let the market take care of it all! Private charity can do the rest.” That’s simple and pure, and works great in bull sessions with other Libertarians. But it will never, ever fly as a serious public policy proposal.
Refusal to see the pragmatic limits of realpolitik is why the Libertarian Party traditionally receives a whopping 2-3% of the vote, despite at least 40% of the population being at least somewhat aligned with their general principles. I’d rather do a little better than that.
Well, we could do with a little less demonizing. Nobody;s burning anything down. The government is displacing market solutions. If your point of view runs to the socialist, then you’ll see government as the thin reed we all cling to because there are no alternatives. If conservative, you’ll see that there are no alternatives because the swamp is choked with government reeds.
I’d like to say you took the words out of my mouth, except I never formulated the words to say it this well.
On what basis do you argue this?
Australians pay about $8,000 for an angioplasty; the average price for an angioplasty in the US ia $28,000. $20,000 more than in Australia, iow three times the Australian price for the exact same procedure.
Ignoring these results when assessing these two situations is, imho, an overly ideological position.
From these outcomes it’s clear that all Government interventions do not have the same result. I’d go further and suggest that the competence, and the purpose, of the intervention is important.
I am amazed Congress has banned Medicare from negotiating directly with pharmaceutical companies for lower prices. Is that for the consumer’s and tax payer’s benefit? Consider:
And yet they do. Why?
Ha! Well so long as you stay away from youtube presentations you’ll be okay.
Here’s wiki on Australian health care. And some comparative data from SBS which focuses on cost and doesn’t look at quality, which I think is a defect – though it uses life expectancy as a rough guide.
The really old-school system was for people – especially lower-income people – to join mutual aid societies, purchasing discounted bulk medical care in the form of “lodge practice”, nursing care, or society hospitals. These societies also offered life insurance benefits, disability benefits, etc, for members and their families.
Many benefits could be demanded as if by right as long as members met minimum requirements to remain in good standing (met certain behavioral standards, paid membership dues – or during hardship, successfully petitioned to have dues waived).
Mutual aid societies with benefits affordable to the very poor and marginalized existed. Moreover, receiving care beyond the entitlements of mere membership happened frequently. So, for example, if members in good standing had children born, through no fault of their own, with chronic illnesses, the society would often arrange extra care for those children beyond the typical membership benefits.
Mutual aid societies weren’t a panacea, and some offered benefits we would today consider rather meager. But these societies tangibly improved poor people’s lives, and showed that individual families needn’t be left entirely to their own devices absent government. There are other alternatives.
Midge, WFB! Long time no see!
Yup. We have a vestige of those in mutual insurance companies. They still have some tax advantages, but they are not very distinguishable from other insurance companies anymore.
Although they do have tax advantages, government has a conflicted relationship with them because they are competition. Government wants people to be dependent on government.
Health sharing ministries appear as if they may be a resurgence of the old mutual aid societies in some ways. Moreover, even absent health-sharing ministries, churches can still offer members some of the same informal services, such as fundraising for a child who has cancer.
True story: my Protestant parents, who had scrimped and saved to move into the tony school district where I was raised, sometimes became enraged at the Catholic families, many of them noticeably better-off than us (for example, able to afford Catholic-school tuition on top of the property taxes), whose yards hosted endless parades of fundraising signs for various parish projects, such as treating one child’s cancer, or sponsoring a class mission trip. How tasteless of the relatively well-off to beg, my parents complained.
My parents were missing the point, I think. These signs were how neighbors advertised their voluntary commitments to each other. No one was ever forced – I don’t even remember non-Catholics facing informal shame for not participating.
Didn’t know about those. Thanks for the information.
The Amish have long operated this way. But as they become a less agricultural society, with greater inequality of income and wealth, that puts new stresses on their way of doing things. It’s probably more of a stress on property insurance (so to speak) than medical insurance. But I met a Mennonite business owner who told how the community helped rebuild when he lost one of his buildings. (These are Mennonites who live much like the Amish, with plain clothing, low tech, horses and buggies.)