Ricochet is the best place on the internet to discuss the issues of the day, either through commenting on posts or writing your own for our active and dynamic community in a fully moderated environment. In addition, the Ricochet Audio Network offers over 50 original podcasts with new episodes released every day.
 Two Things to Remember About Health Care Policy
Two Things to Remember About Health Care Policy

 When trying to formulate a logical, humane health care system, the key is to start from this fundamental understanding: In our wealthy Western countries, we’re not going to let people die in the streets because they can’t afford readily available health care treatments.
When trying to formulate a logical, humane health care system, the key is to start from this fundamental understanding: In our wealthy Western countries, we’re not going to let people die in the streets because they can’t afford readily available health care treatments.
Since everyone knows we aren’t going to turn people away from emergency rooms, a completely free market won’t work. The free rider problem is insurmountable. People can and will choose not to participate in the market until they become sick, and they will then rely on the good will of society to care for them. So the government will be involved in the health care delivery system in some way. Given the free rider problem, it should do so realistically: It should help people at the bottom while keeping government distortion of the market to a minimum.
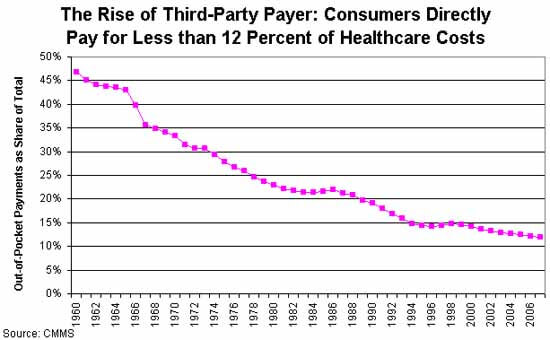 The next thing to consider is the big question: Why is health care so expensive? There’s widespread agreement that third-party payment through insurers is the main problem. There’s no cost control, because neither doctors nor their patients have any incentive to control costs. The only way to gain control over costs is to increase bureaucratic oversight – which adds to the cost.
The next thing to consider is the big question: Why is health care so expensive? There’s widespread agreement that third-party payment through insurers is the main problem. There’s no cost control, because neither doctors nor their patients have any incentive to control costs. The only way to gain control over costs is to increase bureaucratic oversight – which adds to the cost.
Given these two broad parameters, it seems to me that a free-market health care system (or one that’s as free as possible given the first constraint) should begin with universal, single-payer, catastrophic coverage only insurance. That insurance should be very limited in scope to minimize the third-party payer problem.
In a universal catastrophic insurance system, the government would pick up your health care costs, but only if your health care problems reached a threshold such that they were a very significant hardship. This would prevent casual abuse of the system, and it would keep government costs low by eliminating the coverage of routine medical expenses. So: no coverage for routine exams, birth control, small procedures – the things that make up a huge percentage of costs, but should never be paid via an inefficient insurance system. And nothing at all should be covered until you hit your deductible.
To make this palatable to progressives, you can raise the deductible in tandem with income. So a person who makes $20,000 a year might only have to pay for health care until the bills hit $2,000 in a year; a person making $200,000 might be responsible for the first $20,000. Bill Gates might be responsible for the first billion. The numbers and time limits could be negotiated. The important point is that you are responsible for your own health care, but if faced with a health emergency that would bankrupt you, the government will step in. A progressive scheme like this would push more health care into the free market, rather than increasing the scope of government.
Now, would this mean that people would have to pay the deductible out of pocket? Of course not. Employers can offer gap insurance, as can private insurers, on an open market. Gap insurance is much less expensive than full insurance because the insurer’s risk is capped. Pre-existing conditions only cost them up to the cap, so the premium for those would be lower. Because the insurer’s liability is lower for lower-income people (because the cap is lower), insurance would be less expensive for the poor.
People who wish to self-insure could open a HSA and save, say, five times their annual deductible, completely tax-free. This would encourage more people to self-insure to cover the gap, and keep even more of the market out of the third-party payer economy.
This plan would be similar to the health care system in Singapore, a country that spends far less than the US as a proportion of GDP on healthcare, and arguably provides better health care. Singapore also adds a mandatory health savings account, Medisave, to ensure people save enough to pay for the deductible.
Comments?
Published in Domestic Policy, General
I beg to differ. When enough productive, tax-paying folks have a hard time getting their own kids in, things will change.
Your initial socialist data point is not the firmest of truths in this analysis. It’s an opinion, and subject to change. Give it time. “We” will gladly let people go without when we recognize that they made choices too.
You think the fact that we don’t let people die in the streets for lack of basic medical care is a ‘socialist data point’?
Am I to understand that you are in favor of letting people bleed to death in the ER if they can’t pay? Or that we should let the children of poor people die of tonsilitis if the parents can’t pay the bill?
The fact is, we don’t do this today, and never have. The system today has hospitals take in people who do not have insurance or the means to pay and treat them for free. The hospitals consider this bad debt to be overhead and it gets worked into the price of everything else. So you’re already paying for them, and were long before Obamacare came along.
Acknowledging this simple fact goes a long way towards steering you towards the right kind of health care policy.
First, society is not government. Second, when the system fails to work for those who support it, it will stop being supported.
Not controversial.
The health care system is severely distorted by government involvement and regulations. The solution to the myriad of problems and deficiencies caused by government distortions is not more government regulations, which will cause further distortion of the health care markets.
I think you are missing the point – a system like this would be far less intrusive than what exists today. It would leave much more of the healthcare market to private decision-making between doctors and patients. It would restrict government interference to only the most difficult, tragic cases and leave everyone else to fend for themselves.
It would replace Obamacare, the current skewed system of incentives for insurers, the unequal tax benefits for private vs work-related insurance, etc.
Basically, when the left makes an argument for public health care they always fall back on describing the hardest cases – the poor mom bankrupted by a cancer diagnosis. What they don’t talk about is the huge amount of waste in a system that uses insurance to pay for routine care because the government incentives push people in to that type of system. This is the equivalent of using car insurance to pay for oil changes and tire rotations. The government has no business involving itself in that level of care.
A catastrophic health care system leaves the routine care and simple operations and child birth and such to the free market. That’s a lot better than what exists today.
This is a great idea and one I’ve discussed many times with many nuances. The question is whether or not the insurance companies behave and how well th citizens behave. Big Pharma, big Tech, big hospital, big tort all have to do a part. Hard task but worthy.
I agree that realistically we have to start from that point. Not in the abstract, where society could develop other mechanisms, but in the real-world 21st century.
But why single payer? What’s wrong with the tax credit system, which allows a lot more market freedom into the picture and cuts down on the redistributive aspect?
EDIT: Basically, it seems that what you’re suggesting is similar to what Walker and Rubio propose, except that they don’t dictate the terms of the catastrophic coverage, allow different plans to compete, and leave to the individual the responsibility to seek it out. Plus they prevent the need for two systems — if you want to put a little of your own money into it, you can just get a better plan rather than having two plans.
That simply seems vastly preferable from a conservative perspective, and likely to work better too. Or is your contention that so many people will not take the trouble to get (virtually free) insurance that it will still be a drain on the system — that we ultimately won’t accept even that level of basic personal responsibility?
Walker’s plan starts at birth and the credit increases at age 18, so — if we need more government involvement — you could literally push it in the schools.
Am I misunderstanding? What I’m hearing is that government basically covers all the big stuff. That isn’t going to be low cost. And of course, we all know that while every life is of infinite spiritual value, we can’t expend infinite amounts of money to extend every life, though of course I agree with you that we can’t let people die in the streets of routine illnesses. I really like solutions like health care savings accounts. Maybe even mandatory ones and then perhaps government provided for the very poor. There’s incentive to use the money wisely, but to use it for health care. I love the idea of having clinics in places like Walmart for routine stuff like ear infections, so that you only see the level of health care provider you need to see. IOW, you don’t see a doctor for the small stuff. I think clinics for the poor are a great idea as well, but charge a few dollars so that there is some cost and they don’t get overused. There are lots of better, free marketish solutions out there.
As nice as this discussion is. As nice as it is to dream. We are going to single payer. The government will require it and the people will support it because in the end health insurance is too difficult to understand so people want it all off their shoulders.
If it’s done intelligently single payer (but not provider) controls costs by giving consumers some collective bargaining power.
That’s how it works in every advanced country with a hybrid system today – for example Australia, where medical care is at least as good as in the US for the vast majority of things, but where we spend about half the proportion of GDP (10% vs 18% ) on healthcare that the US does.
Why are you so committed to reinventing the wheel?
Single payer does not offer appreciable bargaining power over a multitude of large payers. It’s diminishing returns way before you get to the size of the country.
Isn’t one of the main reason for other western countries having as good of healthcare because they partially free ride on America’s huge healthcare spending?
Doesn’t this all assume that in a free market everyone will be unimaginable bastards?
Isn’t that approximately a socialist assumption?
Look I know as much as anyone that the reason we have stupid unjust way of dealing with market failures is because the vast majority of people don’t understand economics and thus want to declare “so government should just fix it with guns” and leave it at that. And this all Assumes they are real market failures, and not just perceived ones because individuals aren’t as smart as and don’t understand the market.
A completely free market means people are allowed to come up with their own ways to deal with people who can’t afford life saving treatment. And when it really gets down to it, aren’t most life extending treatments that are worth it not nearly as expensive as the end of life treatments that often extend life for it’s own sake without thinking about quality of life and comfort of the patient? The “spend a million dollars immediately to save someone for a decent amount of time and for a relatively high quality of life” does happen, but my understanding is it’s rare.
The doctors can correct me, but trying to use the government for a backstop for these kinds of catastrophes doesn’t seem to serve any purpose other than shutting up people who don’t understand medicine and don’t understand the market, including the penchant that people have to donate to funds to save none other than those people we’re worried about.
Can someone explain to me why the old system, where you had a kind of catastrophic coverage – limited – if you were poor by going to the hospital emergency ward, was inferior to this new proposal. The better off members of society pay higher rates to use the same hospitals to defray the cost of what amounts to the hospitals’ charitable work. Otherwise, everyone remains responsible for obtaining their own healthcare with little help – save for Medicaid, I guess, though, when I looked once, the yearly cost for Medicaid coverage was around $10K, so I may not understand that system.
Under the old system, you could be wiped out with a catastrophic illness. Tough for the unlucky, but that’s life. If you had reason to expect you might be prone to such illness, you might take out CI insurance, if you had the foresight and wherewithal. Otherwise, tough luck.
Does it all come down to the proponents of these plans preferring to eliminate these tragedies?
PS. My brother five years ago got an MRI from a private imaging clinic for $400 cash. Had he had the MRI performed at a similar clinic paid for by his current HMO, that HMO would have been billed well over $1000 (but might have paid appreciably less) by the clinic. Why is this? Paperwork? Is this a massive market distortions going on, or something else?
I am astounded at how much pushback these two statements are receiving. Seriously, no healthcare safety net? It’s no wonder we can’t sell these ideas…if you don’t already agree it just looks selfish and judgmental–you made bad choices, sucks to be you.
What if someone lives in a dysfunctional community? What if they are a drug addict or some other undesirable? Are we here to determine their worth to receive treatments? Isn’t the logical outcome of this eugenics?
I get that people are fed up with healthcare and the distortions of government in the market…but this line of argument (people made choices and must live with the consequences) will never win an argument. It leaves us basking in our own self-righteousness and self-proclaimed wisdom.
<rant off>
A physician friend of mine runs a small dermatology practice. He keeps a full-time employee to do nothing but deal with insurance. He contends that if we all paid as we go for the small stuff and used insurance only for the big stuff, things would improve dramatically.
He also believes the next big wave in doctoring will be concierge medicine.
Isn’t the emergency room policy a healthcare safety net of sorts? This was the way of the past. What was wrong with it exactly?
I agree with your first assumption, but disagree that it requires a government solution. Private charity is much preferable to government solutions because even though the charity doesn’t apply a financial cost to the recipient it does apply a psychological cost in the form of obligation and gratitude that government entitlements do not. In that way charity is just another market payable in a different currency which helps both recipient and customer to seek value, wheras government entitlements are seen as an obligation owed to the recipient and do not provide incentive to seek value. In fact, it has the reverse incentive of making recipient and providers seek maximum payout not maximum value.
How does this US healthcare spending explain me paying less for procedures (like an angiogram or bypass surgery) than you do? There’s no connection.
I understand the ideological urge to believe that you aren’t being ripped off, but I think that you are.
It’s a very expensive way of providing a safety net.
Prove it. I doubt it is more expensive than other ideas floated here. And it has the huge advantage to conservatives in that government is not involved at all in the process.
ripped off by whom? We know what the profit margins are in all industries in the US. There is nothing outrageous in these margins in any of the health related industries. We get Canadiens coming to the US all the time to have procedures much more quickly because they are very much delayed in their own country. So maybe we are just paying extra for a more responsive system. Your bias seems very much on display here.
I think your proposal is very sound, but you need to fill in a few more points between the first sentence here and the second to make your proposal palatable to a stringently antigovernment audience like the one here. I think the intervening steps go something like this:
Everyone knows we are not as a society going to turn people away from emergency rooms or deny them care because they are unable to pay for at least some level of life-sustaining medical care. The free rider problem then arises, because some people will choose to put off obtaining care until they need it. Others will be born requiring lifelong care or will acquire a life-threatening medical condition while they are still children.
Historically, these needs have been met largely by private charity, but the rapid expansion of our ability to extend life has outstripped the ability of private charity to handle those needs, at least at the moment. It may be that at some future time, private charity could rise to the level of meeting those needs. But in the short term, some government payment for medical care is probably necessary and is certainly required to make any proposed health care system politically palatable to the electorate.
Because in America, (a) the smartest and hardest-working people have options that pay way better than medicine (ex. investment banking), so we have to pay doctors more to attract the best to medicine (quasi-rent 101); and (b) our crazy government insurance system drives up costs.
I don’t think doctors are overpaid. If you look at the results they get, and the time they have to put in to become and continue to be physicians, it’s a bargain. The problem is that the government has about eight thousand Medicare reimbursement codes, and since the government gets the best price, everyone who accepts Medicare has to bill that way. So instead of just billing by a multiple of the doctor’s time (ex. salary times three), we bill by procedure. That’s expensive.
The problem is that there are a lot of illnesses that cannot be adequately treated in an emergency setting, or for which the treatment is massively more cost-effective in an outpatient setting. Contrast, for example, good blood sugar control for a diabetic to treating the diabetic with lengthy hospitalizations for complications of poor blood sugar control.
There are lots of people who are born with illnesses or who develop them in childhood.
Do you really want to tell the eight-year-old Type I diabetic, “sucks to be you. Your life expectancy is short AND you can expect to be destitute your whole life because you will be uninsurable and have to pay for any health care out of pocket?
Massive, massive market distortions for sure. There has also been an absolute wall of opposition created by all the physicians’ groups (and I speak for my group, the radiologists, in particular) to competing on quality. There is simply no way to know whether your brother had a dreadful, 1990s level scan with horrible images, or whether he had a state-of-the-art scan read by a subspecialty trained radiologist. Nor is there any way to know whether the facility with which the HMO had a contract would have done better or worse.
Wait a minute did not Obama claim that every year there was a thousand dollars in additional insurance premiums paid on every policy from free riders? Then did not an extensive study come out and say it was more like $100 dollars?
I am sorry if I only have to pay another $100 or $200 dollars a year because of free riders, I will gladly pay that because that is pennies compared to how much the government drives up cost.
So I reject the premiss we have we have a free rider problem. Yes in absolute terms it is tens of billion of dollars. In % of total medical care, it is a single digit expense. I call that a minor issues not a problem that the whole industry and a majority of medical laws should revolve around. You are making a mountain out of a mole hill. The FDA, the Judaical system, and Insurance (including governmental) are the elephants in the room screening in terror at the little mouse called free riders.
I can’t speak to these procedures in particular, but I think in general the idea is that the US as a society has invested a huge amount of our resources into developing care models, including surgical and nonsurgical procedures, that are then copied by the rest of the world. That is becoming somewhat less the case in the modern world, because our government has gotten involved in health care and in the name of protecting patients has massively increased barriers to research and innovation. That fact may give you some idea about why it may be much less desirable for the US government to take over health care than it has been for the Australian government to do so.
The scan was equally good. The price difference comes from something else. I would say that his experience when paying with cash was quicker than when paid for by the HMO
Related to several of the above comments: we can easily create a solution that doesn’t screw kids whose parents can’t pay for them while retaining a lot of the benefits of a free-market system. Basically, we pay for kids (or parents pay for their kids, up to a maximum percentage of their income, and we pay the rest), and once the kid becomes a legal adult, he has the option of purchasing insurance (high-risk pool if necessary; college insurance for those in college; catastrophic for everyone who doesn’t have a lot of money).
Then we continue with the rule we’ve had since 1996, but expand it to private plans: if you are continuously insured (or uninsured for less than 63 days), you can’t be denied for preexisting conditions. That applies equally to the scions of wealth and the kids who pay their $30/month catastrophic care premium with their barista wages.
Of course, that would also involve the government repealing the new law about only charging middle-aged people three times what young people are charged. Ten years ago, I got an amazing insurance plan for $100/month. Catastrophic for that age group really is about $30/month.
This stuff isn’t hard. It just requires understanding the myriad of distortions the government has introduced into the system.
I think the really huge problem is how to take care of people who have chronic illnesses that develop early in life, and for whom the lifetime cost of care can on an actuarial level be assumed to be more than they are able to put into the system. I suppose you could call it a free-rider problem, but it is not that in the sense of a person sitting around and not buying insurance until it’s required. Historically these people have survived either by getting jobs with large employers and entering large pools of healthier people who basically share the cost, or they have landed in some form of government health care. We’d like to decouple health insurance from employment, but by doing so, we foreclose one of the two major options.
By putting a government safety net in place but allowing people to manage their care until the safety net kicks in, you could give these people a sense of security and at the same time allow some market forces to kick in and drive down the cost of managing these chronic illnesses.
I can remember when there was no health insurance. Doctors were paid in cash and made house calls. A middle class income (with a stay at home mom) could pay the health care cost for the entire family, even extended hospital stays. Then Medicare happened and health care costs started their parabolic rise.
The best solution just might be finding our way back to a free market for health care.